


Testicular cancer affects the young adults when testosterone fluctuations are maximum. About 1% of all malignant tumors are testicular tumors. And 99% of the tumors are malignant.
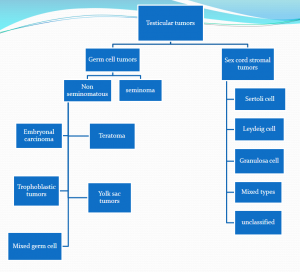
Testicular germ cell tumors comprise more than 90% of testicular cancers. These cancers are strongly associated with a psychological distress and infertility. However, among cancers, testicular cancer is considered the most curable neoplasms among the solid tumors.
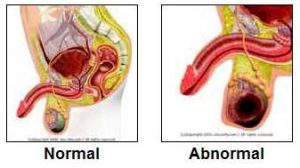

The patient will note a nodule or a painless swelling of the testes. Occasionally, sudden enlargement of a previously atrophic testis may be noticed by the patient.
Testicular cancer is more likely to develop in patients with undescended testis. The risk of cancer is also high in the normal testes in a patient with one undescended testis.
Clinical Features of a Testicular Cancer:
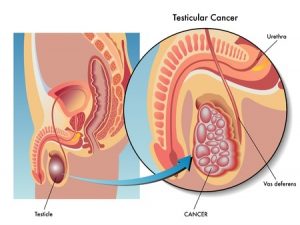
Examination of a patient with testicular cancer will reveal a firm to hard testicular mass which is fixed to the skin and underlying structures. A hydrocele may or may not be present. Inguinal and abdominal lymphadenopathy should also be looked at.

About 40% of the patient will have a dull, aching pain in the lower abdomen, perineal area or scrotum. 10% of the patients can present with acute onset of severe pain in the lower abdomen and or scrotum.
10% of the patients may present with symptoms and signs suggestive of metastasis.
Presentation of a metastatic Testicular cancer
- Lymphadenopathy especially supraclavicular lymphadenopathy
- Shortness of breath, cough hemoptysis (suggestive of pulmonary metastasis)
- Abdominal lymphadenopathy may cause symptoms of intestinal obstruction. A bulky psoas and nerve root involvement due to a retroperitoneal disease may present with lower backache and ill localizing neuropathic pains.
- Skeletal pains due to skeletal metastasis
- Spinal, cerebral or nerve root involvement may cause focal weakness and neurological deficits
- Patients may present with deep vein thrombosis in the iliac, femoral and renal
- Gynecomastia may develop in men especially young boys with Leydig cell tumors. Other patients may present with impotence, loss of libido, a testicular mass and gynecomastia.


Diagnostic evaluation of a Testicular Cancer:
- Scrotal ultrasound
- Radiographic testing,
- Measurement of serum tumor markers
- Radical inguinal orchiectomy
- Retroperitoneal lymph node dissection.
Testicular biopsy is not performed as part of the evaluation due to concern that it may result in tumor seeding into the scrotal sac or metastatic spread of tumor into the inguinal nodes.
Scrotal ultrasound:
- A scrotal ultrasound can distinguish intrinsic from extrinsic testicular lesions
- Seminomas appear as well-defined hypoechoic lesions without cystic areas
- Nonseminomatous germ cell tumors (NSGCTs) are typically inhomogeneous with calcifications, cystic areas, and indistinct margins
A scrotal ultrasound cannot replace radical inguinal orchiectomy for the determination of histology and stage of cancer.
All patients with a solid, Firm Intratesticular Mass that cannot be Transilluminated should be regarded as Malignant unless otherwise proved
Role of the CT scan:
- Regional metastases first appear in the retroperitoneal lymph nodes.
- Although CT is the imaging modality of choice to evaluate the retroperitoneum, false negative rates as high as 44 percent have been described
- Occult micrometastases are responsible for most of these false negatives
Serum tumor markers:
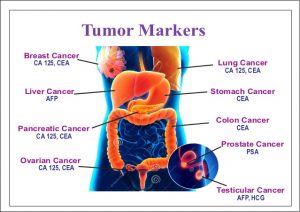

- Three serum tumor markers have established roles in testicular cancer:
- alpha-fetoprotein (AFP), the beta subunit of human chorionic gonadotropin (beta-hCG), and lactate dehydrogenase (LDH).
- Serum levels of AFP and/or beta-hCG are elevated in 80 to 85 percent of men with NSGCTs (Non-seminomatous germ cell tumors), even when nonmetastatic.
- In contrast, serum beta-hCG is elevated in fewer than 20 percent of testicular seminomas, and AFP is not elevated in pure seminomas.
- Serum beta-hCG concentrations above 10,000 mIU/mL occur only in GCTs.
- Serum AFP concentrations above 10,000 ng/mL occur almost exclusively in GCTs and hepatocellular carcinoma.
Although serum tumor markers are helpful at the time of initial diagnosis of testicular cancer and for prognostication, their main utility is for subsequent follow-up of disease status after primary treatment.

Causes of elevated Alpha fetoproteins:
- Pure embryonal carcinoma
- Teratocarcinoma
- Yolk sac Tumour
- Combined Tumour
Causes of raised Beta HCG:
100 % – Choriocarcinoma
60% – Embryonal carcinoma
55% – Teratocarcinoma
25% – Yolk Cell Tumour
7% – Seminomas
Radical inguinal orchiectomy:
- A radical inguinal orchiectomy should be performed to permit histologic evaluation of the primary tumor and to provide local tumor control.
Retroperitoneal lymph node dissection
- Retroperitoneal lymph node dissection is the only reliable method to identify nodal micrometastases given the high false negative rate with CT scan
Cryopreservation of the sperm:
- Semen cryopreservation should be made available to all men diagnosed with testicular cancer prior to instituting therapy if they wish to preserve fertility.
If possible, a baseline sperm count and sperm banking should be performed prior to the radiographic diagnostic evaluation in order to avoid radiation exposure of the sperm
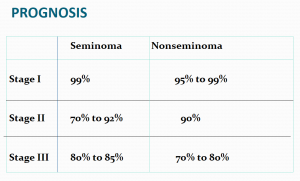
Treatment of Testicular cancer:
- Treatment should be aimed at one stage above the clinical stage
- Seminomas – Radio-Sensitive. Treat with Radiotherapy.
- Non-Seminomas are Radio-Resistant and best treated by Surgery
- Advanced Disease or Metastasis – Responds well to Chemotherapy

Read More …
- Cervical cancer prevention
- Fatty liver increases the risk of liver cancer by ten times
- Diagnose this patient with fever and lymphadenopathy
- Major causes of tiredness and fatigue
- Sexual disorders in men