Lumbar puncture procedure is commonly performed in patients with neurological diseases. It is performed for both diagnostic and therapeutic purpose. Here we discuss how a lumbar puncture is performed and what are the indications and contraindications for a lumbar puncture.
How to perform a Lumbar puncture Procedure?
Before proceeding to the steps of a lumbar puncture procedure, we should have all the necessary equipment for the procedure and obtain proper consent from the patient.
- Spinal tap (lumbar puncture) tray,
- Antiseptic solution,
- Sterile drape,
- 3-way stopcock,
- A spinal fluid pressure manometer,
- Lumbar puncture needle (various sizes),
- Fluid collection tubes (3 or 4),
- Gloves, sterile (physician), Gloves, nonsterile (nurse),
- Local anesthetic,
- Adhesive bandage, and
- Gauze Sponges.
Positioning the patient properly makes the procedure easy …
.jpg)
A lumbar puncture procedure can be performed best in the lateral recumbent position. However, an upright sitting position can be used in some patients.
Identifying the site for needle insertion …
Palpate both iliac crests. A line joining the iliac crests is a guide to the fourth vertebral body. Identify the interspaces by palpating the spinous processes.
The space between the third and fourth lumbar vertebra or 4th and 5th lumbar vertebra can be safely used for CSF drainage as the spinal cord terminates above this level.
Disinfect the site …
The patient should be made to lie in a fetal position. The overlying skin should be cleaned with a disinfectant like povidone-iodine and alcohol.
Before inserting the needle, let the antiseptic dry completely. A sterile drape with an opening for the procedure should be placed.
Local anesthetic should be infiltrated into the area prior to inserting the LP needle.

The spinal needle should be inserted into the subarachnoid space. The needle should be directed towards the umbilicus of the patient and inserted slowly till resistance suddenly decrease. The stylet should be removed to check for CSF.
When CSF starts to flow through the needle, a manometer should be attached to measure the pressure.
What is the normal intracranial pressure range?
The normal CSF pressure is 5 to 15 mmHg or 10 to 18 cm of water.

What are the causes o raised CSF pressure?
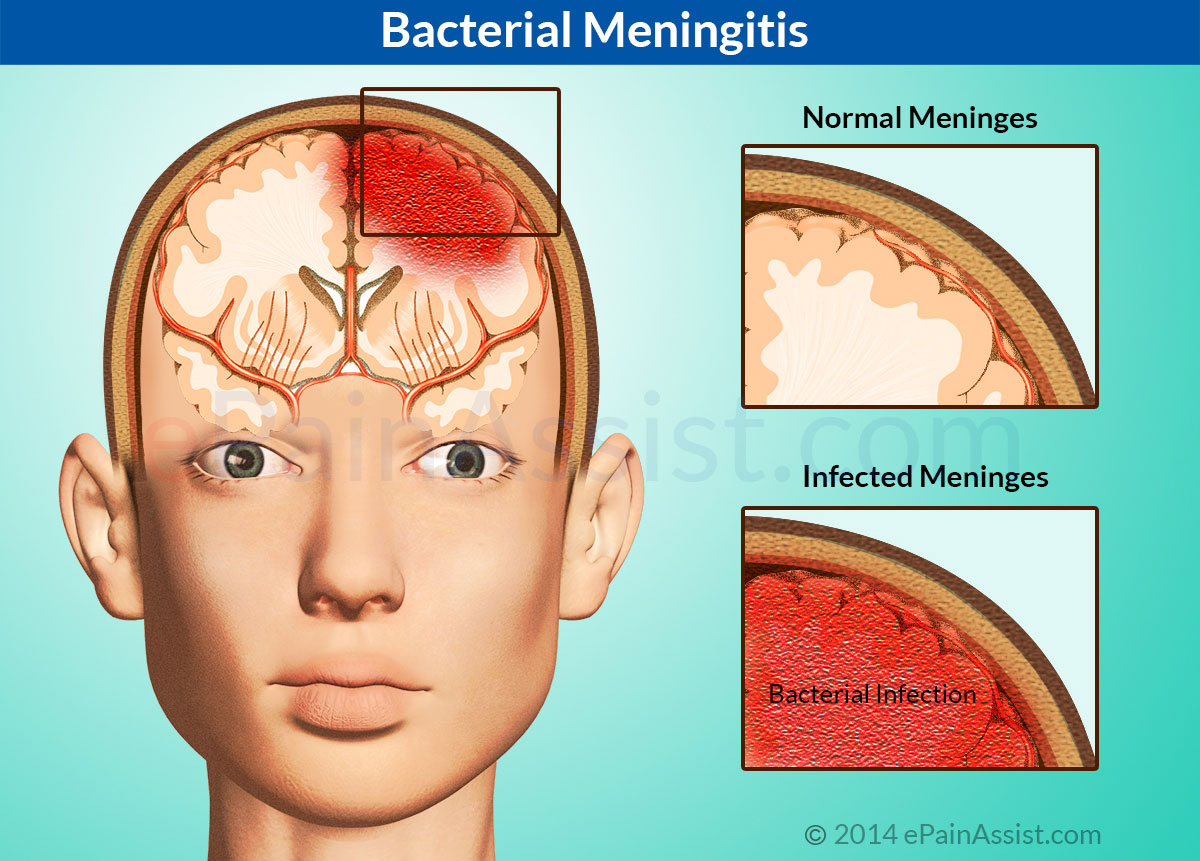
Raised intracranial pressure may be caused by infections of the brain or the surrounding coverings (the meninges) like meningitis, encephalitis and brain abscesses.
Raised intracranial pressure can occur after trauma, brain injury, strokes, intracranial bleeding, intracranial tumors, and hydrocephalus.
In young obese females, especially using oral contraceptive pills, benign intracranial hypertension or pseudotumor-cerebri may cause a headache due to a raised intracranial pressure.
What are the causes of low CSF pressure?
The most common cause of intracranial hypotension or a low CSF pressure is CSF leak. It may also follow spinal procedures and surgeries and conditions with chronically low systemic blood pressure and dehydration.
Next, collect the CSF …
The CSF pressure is then collected in the tubes marked as Tube #1, Tube #2, Tube #3 and Tube #4.
Which bottle? which Test?
Use bottles 1 for the chemical and serologic test (the tube may be frozen).
Tube #2 may be sent to the microbiology lab for cell count and culture (store at room temperature).
Send Bottle # 3 for hematology.
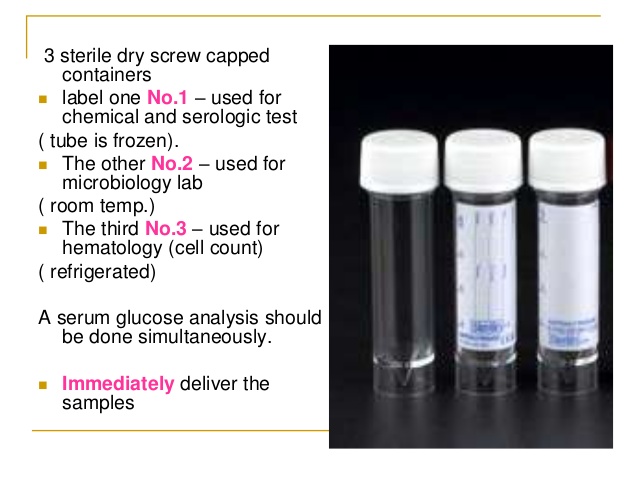
In cases where cell cytology is requested, Bottle #4 should be sent for cell cytology.
Never Aspirate the CSF as it may increase the risk of herniation of the brainstem leading to death.
Before removing the LP needle, insert the stylet.
Ask the patient to drink a glass of water or any fluid and lie down for about half an hour to reduce post-lumbar puncture headache.
What are the indications for a lumbar puncture?
Lumbar puncture is indicated to diagnose CNS infections like bacterial, viral, fungal and tuberculous meningitis.
It is also useful in diagnosing autoimmune and immune-mediated diseases like GBS, and multiple sclerosis and certain malignancies.
It may be used for therapeutic purposes in diseases with raised intracranial pressure like pseudotumor cerebri and hydrocephalus.
In certain malignancies importantly leukemias, lumbar puncture is performed for intrathecal administration of chemotherapeutic agents.
Blood in the CSF can be either due to a traumatic tap or because of subarachnoid hemorrhage. In a subarachnoid hemorrhage, xanthochromia develops after two hours of the bleed.
Xanthochromia is the yellow supernatant, representative of the hemoglobin degradation product. Xanthochromia is highly sensitive if performed after 12 hours of SAH.
When is a lumbar puncture contraindicated?
Lumbar puncture should be delayed in the presence of a raised intracranial pressure as there is a risk of brain herniation. Coagulopathy and thrombocytopenia may lead to unstoppable bleeding at the site.
A hematoma or blood in the CSF may lead to pressure effect on the spinal cord causing nerve compression and lower limbs weakness or paralysis.
Infection of the overlying skin or an epidural abscess is another contraindication as the risk of introducing infection is high.
Complications of a lumbar puncture:
CSF drainage is associated with a POST-LP headache, a very common complication of lumbar puncture.
It may be reduced by hydrating the patient, keeping the patient in a supine position for at least half an hour after the procedure and giving paracetamol to the patient.
Introducing infection because of the infected overlying skin or performing the procedure in an unsterile environment is an uncommon complication.
Similarly, bleeding at the lumbar puncture site, cerebral herniation and radicular pain manifested by a sharp pain radiating down the leg may complicate the procedure.
Lumbar puncture should not be performed in patients in patients with coagulopathy and those actively bleeding.
Patients with a platelets count of less than 50000/ul or an INR of more than 1.4 should not be advised to undergo the procedure without correcting them first.
Warfarin and Aspirin should ideally be stopped 5 to 7 days prior to the procedure. Heparin in therapeutic doses should be stopped at least 12 hours prior to the procedure.
Patients on prophylactic subcutaneous heparin need not stop heparin if the dose is less than 10000 IU.