



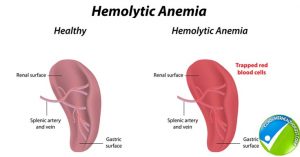
Hereditary spherocytosis is a familial hemolytic disorder with variable clinical features. It is the most common congenital hemolytic disorder due to a defect in the red cell membrane.
Hereditary spherocytosis Inheritance:


Any of the Six genes that code for proteins responsible for maintaining the membrane skeleton may be defective.
Spectrin deficiency leads to loss of erythrocyte surface area, which produces spherical RBCs that are more fragile and easy to break.
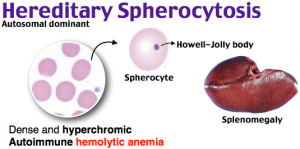
In 75% of the patients, the pattern of inheritance is autosomal dominant. Most of the remaining 25% have autosomal recessive pattern while some patients may acquire the disease de novo via genetic mutations and pass on the genes to the next generation in an autosomal dominant pattern.
Hereditary spherocytosis symptoms:

Mild disease:
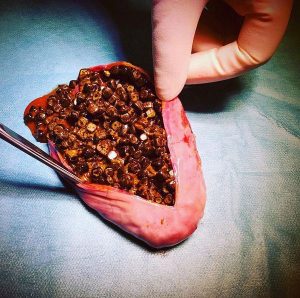
20 – 30% of the patients have mild disease. They may remain asymptomatic, have no or mild anemia and jaundice. The spleen may be mildly enlarged with a mild degree of reticulocytosis.
Moderate disease:
More than half (60 -75%) of the patients have a moderate disease. These patients have mild to moderate anemia, modest splenomegaly, and intermittent jaundice. These patients are diagnosed in their early childhood or even in infancy.
Severe Hereditary spherocytosis:
Up to 5 % of the patients have severe disease. These patients have severe hemolytic anemia and are usually transfusion dependent. Furthermore, they respond partially to splenectomy.

Patients with the severe disease usually have an autosomal recessive pattern of inheritance. Thus, the parents may be asymptomatic
Hereditary spherocytosis complications:
Kernicterus:
Neonates with HS may develop marked jaundice leading to kernicterus. Identifying the disorder and urgent treatment with exchange transfusion may prevent permanent neurological deficits.
Aplastic crisis:
Patients with hs especially children may develop aplastic crisis after a viral infection, specifically, infection with a parvovirus B19.
Children are also prone to develop megaloblastic anemia because of poor dietary habits/ folate deficiency.
Gallstones:

Patients, especially with chronic ongoing hemolysis and those above the age of ten years, develop pigment gallstones. Some patients with mild to moderate disease may be picked up after they are being investigated for the cause of gallstones, jaundice, and anemia.
An interesting observation is the disappearance of spherocytic red cells and normalization of osmotic fragility after the patients develop obstructive jaundice.
Other complications of hereditary spherocytosis include leg ulcers, osteomyelitis, and priapism. Myopathy, Spino-cerebellar disorders and hypertrophic cardiomyopathy have also been associated with hs.
Hereditary Spherocytosis investigations:


Patients have anemia of varying degrees and moderate (5-20%) reticulocytosis. Because of the loss of cell membrane, the mean corpuscular hemoglobin concentration increases. Characteristic spherocytes can be seen on peripheral smear.
Patients can also have pseudohyperkalemia.
Other diseases in which spherocytes can be seen:
- G6PD deficiency
- Hb H disease
- Autoimmune hemolytic anemia
- Mechanical hemolytic anemia or microangiopathic hemolytic anemia as well as sepsis especially clostridial sepsis.
Specific diagnostic tests include:
- Osmotic fragility test:

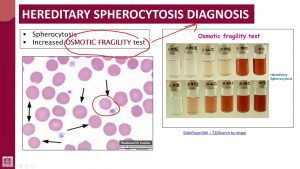
the concept of osmotic fragility is as if you are blowing a balloon. A small balloon will burst after minimal air is blown into it while a large balloon does not burst if the same amount of air is blown into it.
Similarly, normal cells have a large surface area than the red cells in HS. Thus, if red cells of a patient with hereditary spherocytosis are put in a hypotonic fluid, they will easily burst. Osmotic fragility has a sensitivity of 60 -85% in diagnosing Hereditary spherocytosis.
- Many other tests have been developed to diagnose the condition accurately. These include cryo-hemolysis, ektacytometry, acidified glycerol test, and flow cytometry.
Hereditary spherocytosis treatment:
Folic Acid supplements:
All patients with hereditary spherocytosis should be on lifelong folic acid. Folic acid prevents megaloblastic anemia in patients with hereditary spherocytosis.
Red cell transfusions:
Patients with anemia especially a hemoglobin of less than 8 gm/dl or those with a Hemoglobin of less than 10 gm/dl who are symptomatic require Red cell concentrate.
Other patients who should be treated with transfusion support earlier include those with heart diseases, kidney diseases, infections, and other comorbid conditions.
Hematopoietic stem cell transplantation has been successful in some cases.
Splenectomy:
Splenectomy is usually curative except in the autosomal recessive forms. In children, splenectomy should be deferred till the age of six years since the risks of infections are high.
Henceforth, all patients should be vaccinated especially against the encapsulated organisms at least six weeks before (or two weeks after) splenectomy. These vaccinations include:
- Pneumococcal vaccine
- Meningococcal vaccine
- Hemophilus influenza vaccination
Splenectomy should also be deferred in patients with mild disease (hemoglobin of more than 11 gm/dl).


Where expertise is available, laparoscopic splenectomy is a preferred procedure.
Can splenectomy fail to control the disease?
Other than the autosomal recessive disease, other factors may lead to ongoing hemolysis. These include:
- an accessory spleen,
- accidental autotransplantation of splenic tissue into the peritoneum during surgery also called as splenosis.
- Another hemolytic disorder
Failure to observe Howell-Jolly bodies on a peripheral smear may indicate the presence of functional splenic activity.
What changes are expected in a patient who has undergone splenectomy?

- Hemoglobin should increase
- Reticulocyte counts should drop
- Howell-Jolly bodies and target cells may be seen in the peripheral smear
- Leukocytosis and thrombocytosis is expected
Furthermore, patients can die of fatal sepsis caused by encapsulated organisms if not treated promptly.