



Facial hair in women can be mild and be unnoticed but in the majority of young females is very embarrassing. Facial hair in women can be an isolated problem or part of a systemic problem of hyperandrogenism.
When it is part of a systemic disease, it is called hirsutism. Hirsutism is defined by the presence of excess hair growth in androgen-sensitive areas like the upper lip, chin, mid sternum, upper abdomen, back, and buttocks.
Hirsutism and Hypertrichosis:
Hirsuitism should be differentiated from hypertrichosis. Hypertrichosis is the term used to describe excessive hair growth of androgen-independent areas i.e. the hair growth is prominent in non-sexual areas.
Hypertrichosis is commonly familial but can be caused by systemic disorders like hypothyroidism, anorexia nervosa, malnutrition, porphyria, dermatomyositis, and certain drugs like phenytoin.


Although women with hirsutism typically present because of concerns regarding unwanted, excessive hair growth especially facial hair, most also have an underlying endocrine disorder that should be identified.
Causes of excessive facial hair in women:
The following are the most important causes of excessive facial hair in women.
- Polycystic ovarian syndrome
- Idiopathic hirsutism
- Congenital adrenal hyperplasia
- Drugs (danazol and minoxidil)
- Hyperthecosis
- Ovarian tumors
- Adrenal tumors
- Severe insulin resistant syndromes
- Hyperprolactinemia and
- Cushings syndrome
Polycystic ovarian syndrome:


Polycystic ovarian syndrome is the most common cause of facial hair in women. It is characterized by irregular menstrual cycles, features of androgens excess (like acne, deep voice, male pattern baldness, and facial hair) and ovarian cysts.
The major defect in PCOS is the imbalance of androgens and estrogens. When androgens are in excess, females tend to develop excess facial hair, deep voice, masculine features, and menstrual irregularities.
The other hormonal abnormalities associated with PCOS are increased insulin (hyperinsulinemia) in the body, increased insulin resistance in the body leading to diabetes, abnormal fat metabolism (dyslipidemia) and obesity. >50% of the females are obese and have metabolic syndrome.
Metabolic syndrome is characterized by diabetes or pre-diabetes, hypertension or pre-hypertension, obesity, and dyslipidemia (triglyceride levels > 150 mg/dl and HDL <50 mg/dl). Hypothyroidism is also a common occurrence in patients with PCOS.
Patients may also present with excessive snoring, daytime sleeping and features of obstructive sleep apnea.
Most patients are diagnosed when they present for evaluation of infertility. In fact, one of the most important causes of female infertility is PCOS.
Treatment includes weight loss, metformin, anti-androgens, treatment of acne and infertility.
Idiopathic Hirsutism:
When a cause of facial hair in women is not found, it is termed as idiopathic hirsutism. These patients have normal menstrual cycles and normal serum androgen levels.
Up to 90% of patients with idiopathic hirsutism fulfill the latest Rotterdam criteria of PCOS. This criterion incorporates either clinical or biochemical evidence of androgen excess. So, patients may have normal androgens despite clinical features of hyperandrogenism.
Congenital adrenal hyperplasia:
Most Patients with Congenital adrenal hyperplasia have excess androgen production. When there is a block in the cortisol and aldosterone synthesis pathway, the metabolites i.e. precursors are converted into androgens.
CAH is usually diagnosed in childhood. The non-classical forms may be missed and may present in adulthood with facial hair, menstrual irregularity and features of androgen excess.

Patients may present with primary or secondary amenorrhea but the classic features of salt wasting like hypotension, hypoglycemia and hyponatremia and hyperkalemia in classical 21 hydroxylase deficiency ( or hypertension, hypernatremia, and hypokalemia in 11 hydroxylase deficiency) are absent.
Drugs causing excessive facial hair in women:
Androgen therapy (testosterone or DHEA) may be associated with hirsutism. Danazol, a drug commonly used in the past for the treatment of endometriosis, is also associated with hirsutism.
Similarly, Minoxidil, initially used for the treatment of hypertension, is now only used for baldness and alopecia. Hair growth was seen to be a major side effect of this drug.
Hyperthecosis:
Hyperthecosis is a nonmalignant ovarian disorder. It is characterized by increased production of testosterone leading to markedly increased serum testosterone concentrations.
The disorder is still considered by some as part of the spectrum of the polycystic ovarian syndrome. It is characterized by excessive facial hair growth and marked virilization.


Ovarian tumors:
Excessive facial hair can also be caused by some serious diseases like androgen secreting ovarian tumors. These patients present with rapid onset of virilizing features like acne, facial hair and hirsutism, deep voice, and menstrual irregularities.
These tumors can be localized by an ultrasonography and preferably transvaginal ultrasonography, CT or MR. testosterone levels are usually elevated markedly in these patients.
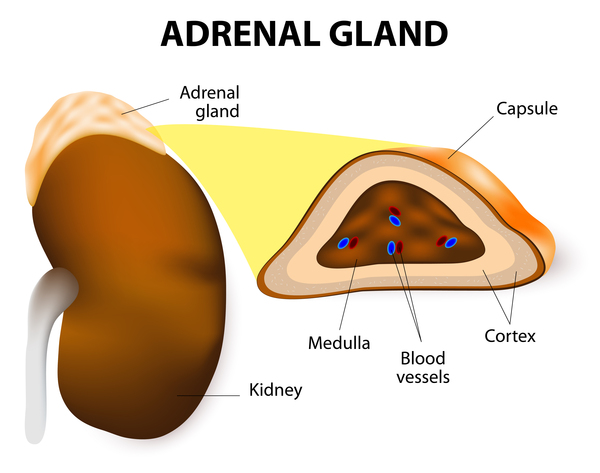
Adrenal tumors:

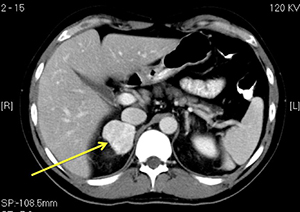
Adrenal tumors are a rare cause of androgen excess. These patients usually have features of androgen excess and hypercortisolism or Cushing’s syndrome.
Patients who develop features of androgen excess and Cushing’s syndrome associated with weight loss and proximal muscle weakness should be investigated for adrenal carcinoma.
Some of the carcinomas may lose the ability to sulfate DHEA, so a normal serum DHEA-S value does not exclude the diagnosis. Nevertheless, an unequivocally elevated serum DHEA-S value is suggestive of an adrenal carcinoma.
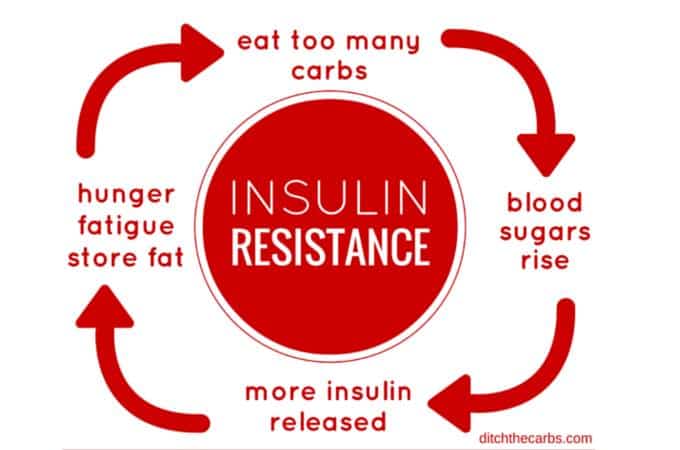
Severe insulin resistance syndromes:
Women who have one of the syndromes of severe insulin resistance and marked hyperinsulinemia often have hirsutism. The marked hyperinsulinemia causes ovarian hyperandrogenism. Insulin also reduces sex-hormone binding globulin, thereby increasing the fraction of free androgens in the serum.

Cushing’s disease:
Cushing’s syndrome and specifically Cushing’s disease is associated with increased adrenal androgen production causing hirsutism. Hypercortisolism should be suspected in women with hirsutism, weight gain, diabetes, hypertension, proximal muscles weakness, recurrent infections, thrush, and purplish striae.
Treatment of hirsutism and facial hair in women
Facial hair in women can cause significant psychological distress, especially in severe cases, in which case treatment is required. In mild to moderate cases, reassurance is sufficient.
Treatment consists of non-pharmacological measures, pharmacological and management of the associated anxiety.
Non-pharmacological measures:
Cosmetic methods:
Physical methods of removing hair or making it less visible (shaving, plucking, waxing, bleaching) can be effective, and their use is reasonable either alone or as a supplement to drug therapy.


Permanent hair reduction:
Permanent hair reduction therapy includes direct or mechanical methods of hair removal, including electrolysis and photoepilation (laser and intense pulsed light).
However, facial hair in women with an underlying hyperandrogenic state is likely to recur because of the continuous androgenic stimulation of hair follicles. Anti-androgen therapy should be part of the treatment regimen in these patients.
Drug therapy for Facial hair in women and hirsutism:
Oral contraceptives with anti-androgenic properties should be used as first-line therapy in patients with hirsutism especially with associated menstrual irregularities.


GnRH analogs can be used in patients who have hypertension or experience hypertension with the use of oral contraceptives. However, since GnRH analogs are very costly, they should not be used as first-line therapy.
Patients with congenital adrenal hyperplasia require treatment with steroids and spironolactone.
Topical therapy:
It is an inhibitor of hair growth, not a depilatory, and must be used indefinitely to prevent regrowth. There is a limited role of topical finasteride or canrenone (the active metabolite of spironolactone)


Facial hair in post-menopausal women:
Postmenopausal women should be screened for an underlying ovarian or adrenal tumor.
Duration of therapy:
After drug therapy is begun, a significant reduction in hair growth may not occur for up to six months. After six months, if the patient feels that the response has been suboptimal, options to consider include a change in dose or drug or addition of a second agent.
Pharmacological therapy is usually continued during the reproductive years as the underlying condition typically persists during this window and hirsutism recurs when treatment is discontinued.
When pregnancy is desired, all pharmacological treatments for hirsutism must be discontinued.
Antiandrogens, in particular, are contraindicated in women trying to conceive because of potential adverse effects on male sexual development.