



This is a “mock exam” question scenario. This question was prepared after we encountered a patient with a bleeding disorder in our ward and was diagnosed with this disease.
This question assesses a student’s knowledge of hematology. The answer will be posted later.
Question – patient with a bleeding disorder
A 20 years old male was brought to the emergency department with a sudden onset of a headache associated with right-sided hemiplegia.
His past history is significant for easy bruisability since childhood including an episode of hemarthrosis of the right knee joint after minor trauma.
He has been transfused with blood products on several occasions in the past. His parents are first cousins and one of his cousins and niece also has a similar problem.
On examination, he had a GCS of 8/15, with an up-going plantar on the right side. Blood pressure was 130/90 and systemic examination was unremarkable.
Labs revealed: Hemoglobin: 10 gms/dl WBCs: 8000/ul Platelets: 190000/ul Prothrombin time: 60/13 APTT: 120/35 Bleeding time: Normal Thrombin time: 60 sec ( <20 sec normal) Chemistry is normal CT brain reveals an intracranial bleed
1. What is the likely underlying hematological diagnosis?
2. What differential diagnosis would you consider?
3. Justify your diagnosis and differential diagnosis?


Before answering the questions lets briefly discuss how to approach a patient with a bleeding disorder …
To secure hemostasis, we require:
- Normal Platelets count and function
- Vessel wall integrity
- Proteins (coagulation factors, collagen, and others)
Primary hemostasis requires:
platelet plug formation at sites of injury.
Tests for primary hemostasis include
Secondary hemostasis requires:
fibrin formation
Tests for secondary hemostasis include
- Prothrombin time (PT)
- Activated partial thromboplastin time (APTT)
- Thrombin time (TT)
- Fibrinogen levels
Next, define whether the bleeding is due to an anatomical defect or a bleeding diathesis. The following important characteristics suggesting a bleeding diathesis should be kept in mind:
- Bleeding following common hemostatic stresses such as dental extraction, childbirth, or minor surgery.
- Bleeding severe enough to require transfusion.
- A family history of bleeding
- Bleeding from multiple sites that cannot be linked to trauma or surgery
Differentiate between defects in platelets and coagulation profile:
PLATELET DISORDER:
- Bleeding localized to superficial sites
- comes on immediately after trauma or surgery
- readily controlled by local measures
COAGULATION DISORDER:
- Occurs hours or days after injury
- Unaffected by local therapy.
- Occurs in deep subcutaneous tissues, muscles, joints, or body cavities.
Let’s discuss the interpretation of the results
Coagulation pathway

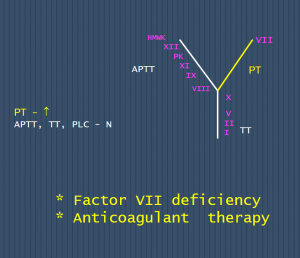
- Abnormal Prothrombin time,
- Normal APTT, TT, and platelets
Diagnosis: Factor VII deficiency and warfarin therapy
2. 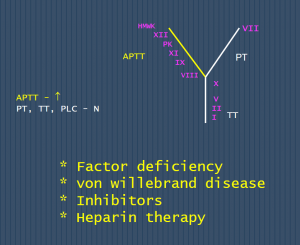

- Raised APTT
- Normal PT, TT, and Platelets
Diagnosis: Factor deficiency (factors XII, HMWK, PK, XI, IX, and VIII), vWD and Heparin therapy
3.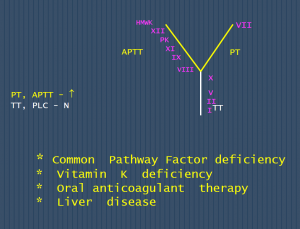

- Both PT and APTT are raised
- Normal Thrombin time and platelets count
Diagnosis:
- Common Pathway Factor deficiency
- Oral anticoagulant therapy
4.

- PT, APTT, and TT raised,
- platelets low
Diagnosis: DIC (Disseminated intravascular coagulation)
Advise FDPs, D-dimers and Fibrin monomers to confirm
Coagulation abnormalities that may be missed
- Factor XIII deficiency,
- Alpha2 plasmin inhibitor deficiency,
- PAI-1 deficiency (PAI-1 is the major inhibitor of plasminogen activators), and
- Scott’s syndrome, a platelet coagulant defect.
- A test for factor XIII–dependent fibrin cross-linking, like clot solubility in 5 M urea, should be ordered when the PT and PTT are both normal but the history of bleeding is strong.
5. 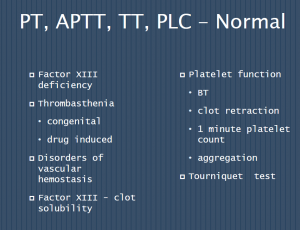

PT, APTT, TT, and Platelets: All Normal
- Factor XIII deficiency
- Thrombasthenia
- congenital
- drug induced
- Disorders of vascular hemostasis
Lastly, causes of abnormally raised thrombin time include:
fibrinogen deficiency or defective fibrinogen (dysfibrinogenemia), liver disease, malnutrition, DIC and Drugs (thrombin inhibitors
Coming back to our patient …
Our patient with bleeding disorder was diagnosed as a case of dysfibrinogenemia.
Raised PT, APTT, TT, and normal platelets count and bleeding time can all be found in dysfibrinogenemia (see discussion for question 3).