Chikungunya is not caused by chicken bites. It has nothing to do with chickens, in fact, it is not even spelled or pronounced like “chicken”.
It is pronounced as CHIK-UN-GUN-YA. Chikungunya word is derived from the Swahili language which means “bends up”, in reference to the stooped posture, developed as a result of Arthralgia (severe joint pains).

Chikungunya fever (CF) is a viral illness caused by an Arbovirus of the genus Alphavirus, transmitted by the Aedes mosquitoes (Aedes aegypti and Aedes albopictus).
It’s the same mosquito that can transmit dengue fever, yellow fever, and zika fever.

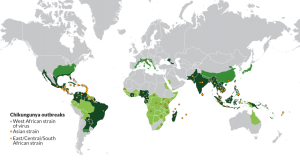
Epidemiology:
It has become endemic in the south and central India. Chikungunya (CHIK) virus first isolated from the serum of a febrile human in Tanzania in 1953.
Chik virus has caused numerous outbreaks in Africa and South Eastern Asia.
MODE OF TRANSMISSION:
It is transmitted by Aedes species Mosquitoes – Aedes aegypti, Aedes albopictus. These are aggressive daytime biters. The major period of activity – sunrise and sunset.
This virus is transmitted only by mosquitoes. The mosquito picks up the virus from an infected person during the viraemic period – within five days from the day of starting of symptoms.
An infected mosquito will remain infected all its lifespan (30 days) and can transmit the virus each time it bites. An infected person cannot spread the infection directly to other persons.
Signs & symptoms:
- Fever Which Can Reach 39°C, (102.2 °F).
- Petechial or Maculopapular Rash Usually Involving the Limbs and Trunk.
- Arthralgia or Arthritis Affecting Multiple Joints Which Can Be Debilitating.
- A headache, Conjunctival Injection, and Slight Photophobia.
- Sudden onset of fever, chills.
- A headache, nausea, vomiting, abdominal pain.
- Low back pain.
Arthralgias:
- The small joints of the lower and upper limbs
- Migratory poly arthralgia – not much effusions
- Larger joints may also be affected (knee, ankle)
- Pain worse in the morning – less by evening
- Joints may be swollen & painful to the touch
- Some patients have incapacitating joint pains
- Arthritis may last for weeks or months.
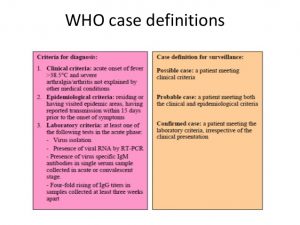
WHO CASE DEFINITIONS:
OUTCOME:
Acute symptoms: resolved in 7-10 days. Mortality is rare (in the elderly). Some patients have relapses of rheumatic symptoms in the months following the acute illness. Chronic illness of varying degrees, with pain persisting for months or years. Lifelong immunity, once one suffers this infection.
Chikungunya Diagnosis:
- REAL-TIME PCR
- ELISA
- PRNT: Plaque reduction neutralization tests (PRNT) are very useful because they are quite specific for alphaviruses and are the gold standard for confirmation of the serologic test result.
Chikungunya Differential diagnoses:
- Dengue fever: Severe back pain with purpuras or active bleeding might suggest dengue fever. Confirmatory laboratory diagnosis is possible.
- Reactive Arthritis: In general, any arthritis that follows a febrile gastrointestinal or genitourinary infection (triggering microbes) is considered a reactive acute inflammatory arthritis if it lasts less than six months. The hallmark feature is enthesitis (is the inflammation of the enthesis, that is the sites where tendons and ligaments insert into the bone) Oral mucosal ulcers are seen.
- Serum sickness illness: Polyarthritis (involving more than 4 joints) may be associated with a serum sickness type reaction caused by vaccine, medication or other viral infections
- Rickettsial disease can present with fever, rash, and joint pains. Confirm by serology.
- Rheumatic fever: More common in the children and presents with fleeting (migratory) polyarthritis predominantly affecting the large joints. Modified Jones criteria should be the basis for diagnosis. Raised ASO titer and a history of recurrent sore throat are other points to be noted.
- Malaria: the patient can present with high fevers and may also complain of joint pains. The periodicity of fever and alteration of consciousness/seizures should prompt diagnosis for malaria
- Leptospirosis: Severe myalgia localized to calf muscles with conjunctival congestion/ or subconjunctival hemorrhage with or without oliguria or jaundice in a person with a history of skin contact to contaminated water would suggest Leptospirosis.
DENGUE AND CHIKUNGUNYA VIRUS INFECTIONS:
Virus transmitted by the same mosquitos. Similar clinical picture. The viruses can circulate in the same areas so co-infection (i-e infection of the same person with both viruses) is possible. Discarding dengue is important, for adequate clinical care that improves the prognosis of dengue.

TREATMENT OF CHIKUNGUNYA:
Supportive care is recommended. Nonsteroidal anti-inflammatory drugs such as naproxen, Paracetamol (acetaminophen). Fluids for symptomatic treatment. Corticosteroids, but not recommended during the acute phase of the disease, as they may cause immunosuppression and worsen the infection.




Chronic arthritis:
In those who have more than two weeks of arthritis, ribavirin may be useful. The effect of chloroquine is not clear. It does not appear to help acute disease, but it might help those with chronic arthritis. Steroids do not appear to be an effective treatment. NSAIDs and simple analgesics can be used to provide partial symptom relief in most cases. Methotrexate has been shown to have benefit in treating inflammatory polyarthritis resulting from Chikungunya, though the drug mechanism is unclear.
Chikungunya Prevention:
Since mosquito is the vector and responsible for transmission of the malarial parasite, one should avoid mosquito bites. This is done by adopting the following measures.
- Avoid outdoor exposure especially between dusk and dawn. This is the time when a mosquito bites.
- Wear clothes with full sleeves and cover yourself to reduce the amount of skin exposure.
- Use insect repellents on exposed Parts of the body.
- Use mosquito nets treated with insecticides at night while sleeping.
Insect repellents recommended by the CDC for reducing the risk of Malaria include DEET (30 -50%).
It is generally protective for 4 hours and is safe for use in children 2 months of age and above. In addition to insect repellents applied to the skin, Permethrin may be used on net and fabrics.
It is available as an aerosol clothing spray. Permethrin is very effective when used for clotting and bed netting. It effectively repels mosquitoes for more than one week even with washing and field use.
Nets dripped with Permethrin are effective for 3 – 20 washes. Long lasting insecticide repellent can remain effective for as long as three years. The use of vaccines in malaria is still debatable.