An elderly patient was referred to Pakistan Institute of Medical Sciences OPD for the work-up of hepatomegaly and weight loss.
The patient, aged 65 years, with no previous premorbid conditions, was alright 8 months back when he developed abdominal pain.
The pain was diffuse, moderate in intensity, and dragging in nature. It was associated with undocumented weight loss, nausea, occasional vomiting, anorexia, and low-grade fever.
The patient also developed lethargy, fatigue, tingling, and numbness of the feet. The patient denied any history of cough, jaundice, melena, or joint pains.
The patient was a watchman at Saudi Arabia, did not admit to any addiction, and belonged to average socioeconomic status.
On examination …
On examination, he was a thin lean patient, with temporal wasting, pallor, and mild pedal edema. There was no accessible lymphadenopathy or skeletal tenderness.
The abdomen was protruded with huge hepatomegaly. The spleen was not palpable and there was no evidence of any free fluid in the abdomen.
Cardiovascular examination was significant for a hyperdynamic precordium. Rest of the systemic examination was unremarkable.
Previous investigations …
The patient’s previous investigations done in other hospitals are as follows:
Blood CBC:
- Hemoglobin of 8 gm/dl,
- MCV: 92 fl.
- WBCs: 16000/ul,
- Sedimentation rate: 126 mm/hour
Liver function tests:
- Bilirubin: 1.4 mg/dl,
- ALT:12 IU/L (normal),
- Alkaline phosphatase: 347 IU/L,
Other chemistry:
- Creatinine: 1.6 mg/dl
- Sodium: 132 mEq/L,
- Albumin: 1.9 gm/dl,
- Proteins: 6.9 gm/dl,
- Calcium: 7.9 mg//dl,
- LDH: 507 IU/L,
- Creatinine phosphokinase: 507 mg/dl,
- Urinalysis: Normal,
- Coagulation profile: normal,
- Alpha fetoproteins: normal
Ultrasound abdomen:
- Hepatomegaly: 20.8 cm,
- Grade 1 renal parenchymal change, and
- Mild abdominopelvic ascites
CECT Abdomen:
- Hepatomegaly: 25.6 cm
- A cluster of calcifications in segments IV a/ IV b of the liver (can represent healed granuloma)
- Simple cysts (right and left lobe of the liver)
- Cholelithiasis
- Right non-obstructing renal calculi
- Mild pelvic ascites
- Bilateral inguinal hernia
- Visualized lung fields: Bilateral pleural effusion and bronchial wall thickening
Echocardiography:
- Ejection Fraction: 60%
- Severe asymmetrical Septal hypertrophy with a small left ventricular cavity.
- Good systolic function
- Moderate MR with vena contracta
- Systolic anterior motion of the mitral valves
Conclusion: Hypertrophic Cardiomyopathy
To Summarize:
An elderly patient with abdominal pain for 8 months, mild anemia, huge hepatomegaly, and Hypertrophic cardiomyopathy.
Can you suggest any investigations to diagnose this patient?
Can you suggest any Diagnosis or differential diagnosis?
Let’s proceed further …
Although few people commented, some answers were excellent.
While this patient was seen in the OPD, we suspected an infiltrative disorder.
What infiltrative disorders can cause cardiomyopathy?
Cardiac Amyloidosis:
- It usually presents in the 6th or 7th decade.
- Patients have a low voltage ECG with pseudo-infarctions and AV blocks.
- ECHO will show a hypertrophic heart with a granular myocardium.
- Cardiac MR will show late gadolinium enhancement
Cardiac Sarcoidosis:
- Presents in the third or fourth decade.
- ECG may show high degree AV Blocks
- ECHO may reveal non-coronary segmental wall motion abnormalities and septal thinning/ thickening.
- Cardiac MR will show a patchy late gadolinium enhancement
Hemochromatosis:
- Presents in the fourth or fifth decade.
- ECG may show non-specific repolarization abnormalities
- ECHO may reveal diastolic disease and global systolic dysfunction.
- Cardiac MR will show a shortened T2 Time.
Fabry Disease:
- Presents in the second through the fifth decade.
- ECG may show an increase in the QRS voltage
- ECHO may reveal concentric left ventricular hypertrophy.
- Cardiac MR will show late gadolinium enhancement of the basal segments of the anterior and inferolateral walls
Danon Disease:
- Presents in the second or third.
- ECG may show an increase in the QRS voltage, short PR interval, and Delta waves.
- ECHO may reveal massive left ventricular hypertrophy with left ventricular outflow obstruction.
- Cardiac MR will show a subendocardial late gadolinium enhancement with septal sparing.
Friedreich’s ataxia:
- Presents in the second or third decade.
- ECG may show non-specific repolarization abnormalities
- ECHO may reveal increased septal thickness.
- Cardiac MR is not used.
Because of our limited knowledge, we suspected the following disorders in our patient:
- An infiltrative disorder:
- Amyloidosis
- Sarcoidosis
- Tuberculosis
- A granulomatous disorder:
- Tuberculosis
- Malignancy
What investigations were advised:
The following investigations were advised:
- A Repeat CECT Chest and abdomen
- A Repeat Echocardiography
- Bone marrow Biopsy
- Serum Protein electrophoresis and immune electrophoresis
- Abdominal fat biopsy
Results of the above investigations:
- CECT chest and abdomen:
- Moderate right sided effusion with adjacent consolidation and collapse of the lung segments
- Multiple soft tissue density nodules in both lungs
- Multiple cystic lesions in both lobes of the liver
- Conclusion: Features (described above) are suggestive of a metastatic disease process.
- Repeat ECHO was consistent with the previous findings
- Bone marrow biopsy: Hypercellular marrow with increased plasma cells (11%)
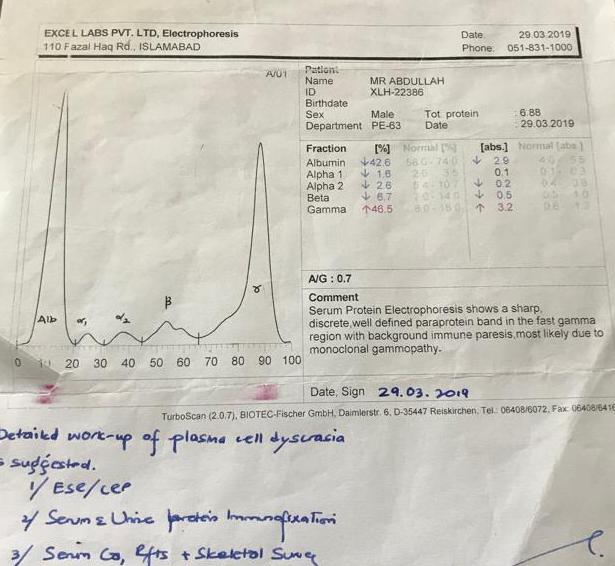
- Serum protein electrophoresis: a sharp M band in the Gamma region as shown below:
- Immune electrophoresis: Increase in the Kappa Light chain ratio as shown below:

An abdominal fat biopsy was not consistent with amyloidosis. Congo red stain and a repeat evaluation of the histopathology report has been requested.
So, we made the final diagnosis of Light chain (Kappa) Myeloma with infiltrative cardiomyopathy.
Oncology consult was requested and the patient was started on treatment. Treatment and discussion of multiple myeloma will be posted in the next article.